30-ABC and the first DCD-NRP in India
Dr (Colonel) Avnish Seth
Indian Transplant Newsletter. 2025 Oct-Dec; 24(4): p4-5
DOI: https://doi.org/10.64384/ITN.2025.063
Print ISSN 0972 - 1568
Online ISSN 3048 - 653X
Download PDF
'Please fasten your seat belts' announced the crew. It was October the 12th 2025. Air India flight IX-1191 from Jaipur to Delhi was ready for take-off. Seated in 30-A, I glanced to my right. Two of the most experienced liver and kidney transplant surgeons in the country were sitting next to me in non-reclining seats next to the toilet. Premium seats for the best in the business, returning from a national transplant meeting! I chuckled to myself at the thought that all of us had overlooked the tiny detail of seat selection. Or was it ordained…
Despite the discomfort, the 40-minute flight gave us an unmatched opportunity to catch up. My colleagues spoke about their journey of completing 1,500 liver transplants in a public hospital and the nuances of teaching robotic kidney transplantation to the Japanese. When I mentioned my thoughts on organ donation after circulatory death (DCD) by using Normothermic Regional Perfusion (NRP), they were all ears.
'Of 18,911 organ transplants done in India in 2024, 82% were from living donors and only 18% were from deceased Donations after Brain Death (BD)', I explained. The donor pool needs to be expanded. In DCD, there is no blood supply to vital organs, as the heart has stopped beating. Time is at a premium and protocols are required for successful organ retrieval and transplantation. The first national summit on DCD was organized by us in association with MOHAN Foundation at Gurugram, way back in 2015. It became clear at the summit that there was provision for DCD in Transplantation of Human Organs Act, 1994.(1) It took us seven more years to convince the nation on its legal, ethical and medical aspects. In 2022, we brought out a position statement from eight societies on enabling Categories IV and V of DCD in India.(2) Categories I and II are difficult in India in the absence of presumed consent.(3) Following the Supreme Court Judgement of 2023 on Withdrawal of Life Support Treatment (WLST), a consensus paper with 12 societies was published on protocols for DCD Category III.(4,5) However, as WLST is not yet being performed as a routine in ICUs, a new classification of DCD is proposed for India (Table).
'Haven't we already done kidney transplantation from DCD in the country?', asked my colleague. I explained that a few centers have done kidney retrieval with super-rapid recovery (SRR). Early graft dysfunction with SRR for DCD kidneys is inevitable, but improves with time. About 30% patients even need support with short-term dialysis, a luxury not available for other organs. Liver transplantation may not work well with SRR as there is ischemic injury to the bile ducts. Perfusing the retrieved liver in machines with blood or hypothermic solutions before transplantation is a good but expensive option. NRP is a technique where oxygenated blood is perfused to abdomen (A-NRP) or thoracic and abdominal (TA-NRP) cavities for up to 4 hours after death, thus mitigating ischemic injury and enabling utilization of organs (Fig 1). I mentioned that National Consortium on NRP was set up in 2024 and 22 experts have been working on developing low-cost hybrid ECMO for India (Fig 2). 'The Consortium did a dry run on NRP in ICU and OT at Manipal Hospital Delhi on 29th March 2025 and we were ready with the protocol', I said.
The discomfort in my blocked sinuses and ears signaled that the plane was descending rapidly. I pinched my nostrils, did the Valsalva maneuver till the ears popped, and sipped some water. Outside, the evening smog hung like a veil, failing in its attempt to mask the bright lights and bustle of the capital. As the aircraft came to a halt, we stayed in our seats and watched passengers leave. When it was our turn, we reached for our handbags and shook hands. Straightening the tie, I pulled on my jacket and walked out. I was ready.
On 6th November 2025, a 55-years educator, bed-bound with progressive Motor Neuron Disease for two years, was brought to our emergency with labored breathing and dullness of sensorium. On arrival, GCS was E4V1M5, respiration 30/min, pulse 115/min, BP 110/70 mmHg. She was afebrile and pupils were equal and reacting to light. Examination of CVS and lungs was unremarkable, and she had features of advance Amyotrophic Lateral Sclerosis. ABG on arrival showed respiratory acidosis with pH 7.14, PaCO2 135 mmHg, Lactate 0.3 mmol/L and HCO3 45 mmol/L. Aligning with the wishes of the patient, the family signed do not attempt resuscitation (DNAR) and she was shifted to ICU on non-invasive ventilation (NIV). Over the next 24 hours, the family expressed their desire to 'let her go in peace' and 'donate organs if possible'. Ms Sukhvinder, our transplant coordinator, explained the steps of DCD and NRP. Besides 'Form 8', an additional consent form created by National Consortium, that included placement of vascular lines and heparin, was used. The Critical Care team, led by Dr Shrikanth, swung into action. Sheaths were placed in both femoral arteries and right femoral vein and Heparin was administered. Once the NRP set-up was complete and the family had spent some time with the patient, NIV was discontinued at 8:13pm. Cardiac arrest occurred at 8:33pm. Following a no-touch period of 5 minutes, femoral arterial and venous cannula were positioned. Extra-Corporeal Membrane Oxygenator (ECMO) with reservoir was used to establish A-NRP. Aortic Balloon was placed in supradiaphragmatic aorta through left femoral access and inflated to prevent blood flow into thorax. Mr Rakesh, our Perfusion Technologist, along with Critical Care team ensured that A-NRP was up and running within 17 minutes. Functional warm ischemia time (FWIT) was 24 minutes. Simultaneously, National Organ and Tissue Transplant Organization (NOTTO) was informed, and alert was sent for open offer on liver and kidneys to all 53 hospitals in National Capital Region. Several hospitals accepted the organs as they had blood group matched recipients in the waiting list, but later backed out as they failed to convince the patients to accept DCD organs. Being the first time in the country, there was lot of skepticism on the viability of organs, and it seemed that there would be no takers.
It was 10:34pm. Only two hours more on NRP were possible and there was no sign of organ retrieval. Time was running out. The wishes of the donor family had to be fulfilled. Thinking of our invigorating discussions in the cramped confines of 30ABC, I picked up the phone and dialed both my colleagues. They quickly understood what was at stake. Without hesitation, retrieval teams for liver and kidneys were dispatched from both hospitals.
We carried out NRP for a total of 4 hours and 10 minutes. Peak lactate of 3.6 mmol/L was seen after 30 minutes into NRP, fell to 2.4 at 90 minutes and reaching a nadir of 1.5 at 4 hours. Liver function tests always remained normal. Urine output was 50-60 ml per hour. Liver and kidneys were successfully retrieved and transplanted. The surgeon commented on the excellent quality of the transplanted liver and bile production. The liver recipient was extubated in 12 hours and was discharged in 2 weeks. The total cost of consumables incurred for A-NRP was only INR 92,165.
Considering the large experience of Critical Care Specialists with ECMO in India, A-NRP offers a viable option for utilization of organs in a setting of DCD. In-house utilization of organs may be the best option as allotment and retrieval of organs with-in 4 hours in DCD categories IV and V, is a Herculean task. The next endeavor in the country will be to retrieve lungs in a setting of A-NRP and finally, to carry out DCD heart and lung transplantation with TA-NRP.
References
1. National Organ and Tissue Transplant Organization (NOTTO). Available from: https://www.notto.mohfw.gov.in/act-end-rules-of-thoa.htm
2. Seth AK, Mohanka R, Navin S, Gokhale AG, Sharma A, Kumar A, et al. Organ donation after circulatory determination of death in India: A joint position paper. Indian J Crit Care Med 2022;26:421‑38
3. Kootstra G, Daemen JH, Oomen AP. Categories of non heart beating donors. Transplant Proc 1995;27:2893 4.
4. The Supreme Court of India Civil Original Jurisdiction. Common Cause Versus The Union of India. Writ Petition (Civil) no. 215 of 2005. Available from: https://main.sci.gov.in/supremecourt/2005/9123/9123_2005_ Judgement_09-Mar-2018.pdf. [Last accessed on 2023 Apr 13].
5. Seth AK, Mohanka R, Mani RK, Asthana S, Attawar S, Dhital KK, et al. Organ donation after circulatory determination of death ‐ Consensus statement. Indian J Transplant 2024;18:247-56.
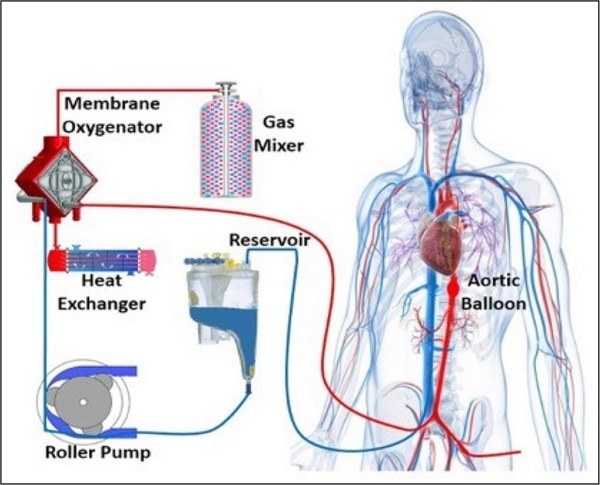
Fig 1: Circuit for Abdominal Normothermic Regional Perfusion
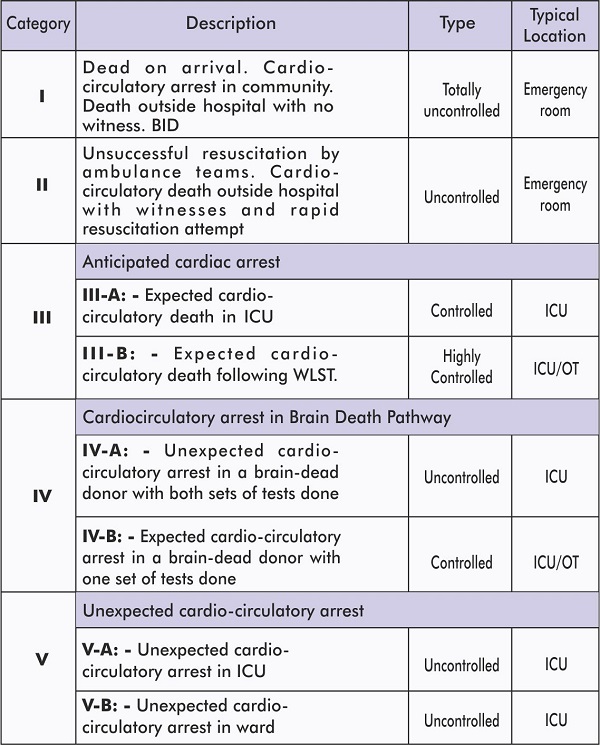
Table: Seth's Modification of Maastricht Classification for DCD in India

Fig 2 : Low cost Hybrid Extra-Corporeal Membrane Oxygenator (ECMO) Circuit with Reservoir
To cite
: Seth A. 30-ABC and the first DCD-NRP in India. Indian Transplant Newsletter. 2025 Oct-Dec; 24(4): p4-5.
DOI: 10.64384/ITN.2025.063
Available at:
https://www.itnnews.co.in/indian-transplant-newsletter/issue78/First-DCD-NRP-in-India-30-ABC-and-the-first-DCD-NRP-in-India-1433.htm
Available at:
https://www.itnnews.co.in/indian-transplant-newsletter/issue78/First-DCD-NRP-in-India-30-ABC-and-the-first-DCD-NRP-in-India-1433.htm
- Copyright © 2026. Published by MOHAN Foundation
