End-of-Life Care in India
Raj Kumar Mani
Indian Transplant Newsletter. 2025 Apr-Jun; 24(2):p4-5
DOI: https://doi.org/10.64384/ITN.2025.034
Print ISSN 0972 - 1568
Online ISSN 3048 - 653X
Download PDF
Introduction: It has come to be a norm for terminally ill patients to spend their dying days in hospitals and ICUs. Aggressive interventions when applied inappropriately in this situation impose enormous physical, emotional and economic burdens on the patient and the family. The quality of dying, therefore needs as much attention as other measures of quality in the ICU. End-of-life care (EOLC) is about the human-centric care of the dying and the grieving, unlike the challenges of resuscitation, rescue and cure in those with a realistic chance of survival. In the West, efforts to integrate end of life and palliative care in ICUs started in the early 1990s. In India, this conceptual shift has been slow to evolve in ICU and hospital practice.
What are the barriers to EOLC in India?
The most formidable barrier is the lack of “death literacy” among both physicians and the lay public. Death is a taboo subject that both baulk at discussing candidly. With the result that the recognition of oncoming death and focus on the needs of the dying get neglected. Death is profoundly difficult to face, although it is widely acknowledged as an inescapable truth. The physicians must skilfully recognize the terminal trajectory of illness and candidly but sensitively share the status with the family. The physician must compassionately support the family through the process of acceptance and appropriate care.
Secondly, there is a lack of ethical awareness and training among healthcare providers. The medical code of ethics is archaic and does not include the ethics of caring for the terminally ill. The medical curricula also fail to address the care of the dying. The entire training is oriented towards curative efforts aiming to “fight till the end”, no matter the phase of the illness or disease trajectory.
Thirdly, the lack of public discourse on the issues around the futility of technologically intensive care in the terminally or incurably ill patients. There is a lack of discussion on how to ensure a good death so far as is possible both in and outside hospitals.
Lastly, there is inadequate direction in National health policy. Although the national policy recognizes the value of palliative care, it is silent about the needs and care of the dying. There is no well-developed national culture that nurtures humane care of the dying except in the state of Kerala that has pioneered community palliative care.
Evolution of end-of-life care in India
At the turn of the millennium, there was little awareness of EOLC in the country. The Indian Society of Critical Care Medicine (ISCCM) published its first position paper in 2005, suggesting an end of life decision-making pathway in the ICU integrating clinical and ethical principles. There was a legal vacuum with only a handful of case laws turning down request for permission to commit suicide for burdensome terminal illness. There was no reference to Do-Not-Attempt-Resuscitation (DNAR) or withdrawal and withholding decisions. The ISCCM approached the Law Commission of India for its opinion on the legal position of foregoing of life support treatment (FLST) decisions in India. The Commission published the 196th draft bill “for the medical treatment of terminally ill patients”. The Bill in its opening lines stated unambiguously that FLST decisions do not constitute active euthanasia, that they do not violate suicide Laws and are legally valid when specific requirements are met. The Bill also disallowed Advance Will believing it to be subject to “misuse”. It proposed decisions to be validated by the High Court which was not practically feasible. Therefore, in a handful of institutions across India the ISCCM pathway was followed for ethical decision-making.
The next milestone on this journey was the Aruna Shanbaug judgement in 2012, where the term of reference was removal of feeding tube from a chronically vegetative patient. For the first time for India, the judgement held “passive euthanasia” or FLST as constitutionally valid. However, it prescribed validation by the high court for withdrawal of artificial feeding in a vegetative patient. The judgement did not address the other scenarios in which FLST was applicable.
In 2015, a professional advocacy was formed called End of Life Care in India Task force (ELICIT) having members from 3 societies- ISCCM, IAPC (Indian Association of Palliative Care) and IAN (Indian Academy of Neurology). It embarked on a vigorous campaign reaching out to other professional group and the lay public to spread awareness. It engaged with legal experts to influence legal developments. It also worked with Indian Council of Medical Research (ICMR) to publish the definition of terms relating to EOLC and a Do-not-attempt Resuscitation (DNAR) guidelines. Many publications in scientific journals and op-eds in major newspapers on EOLC have resulted through ELICIT.
Institutional guidelines and standard operating procedures for EOLC and palliative care were developed by the Manipal Group of Hospitals (The BLUE MAPLE, 2017) and by AIIMS, New Delhi (2020).
The ground breaking judgement was in 2018, Common Cause vs The UOI. Based on the rights of autonomy and privacy enshrined in Article 21 of the constitution, it held FLST to be legally valid when certain conditions are fulfilled. On the same basis, the right to execute a Living Will or Advance Directive (AD) was also held to be valid. What the judgement promoted in principle, it undid in the FLST procedure put forth. It mandated a 3-tier decision-making process involving, apart from 2 medical panels, the District Collector and the judicial magistrate of first class. The procedure was clearly unworkable for the everyday situations in the ICU.
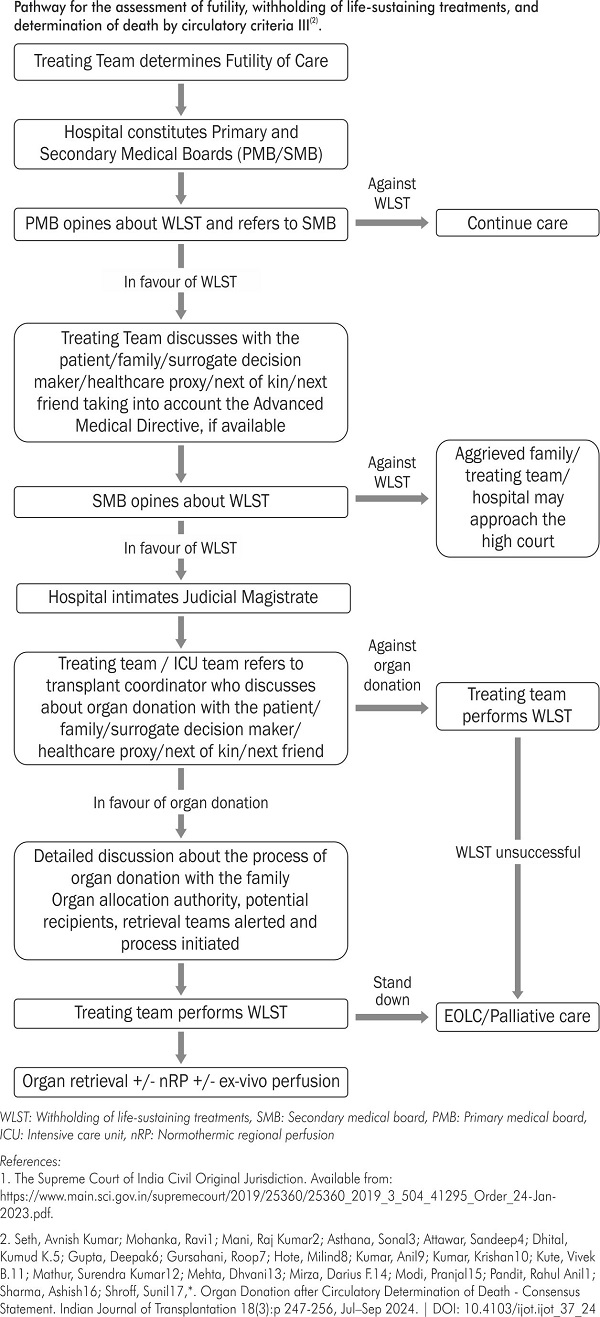
The ISCCM, represented by the Vidhi Center for Legal Policy and supported by ELICIT appealed to the Supreme Court for procedural simplification. In a momentous decision in Jan 2023, the SC allowed simplification of both AD execution and FLST decisions(1). The pathway is similar whether there is a valid AD in existence. A two-tier process was prescribed: a primary medical board in the hospital makes a shared decision with either the legal proxy (where a valid AD exists) or the next of kin. This preliminary step must be validated by a secondary board which includes 3 other physicians, one of whom must be a nominee of the District Health Officer (DHO). All physicians on the boards must have at least 5 years of subject experience. There is nothing in the judgement against having a standing panel of secondary board or having the hospital's physicians nominated by the DHO.
Following this development the ISCCM and IAPC published a position paper on end-of-life and palliative care in Indian ICUs in March 2024. It integrates the latest ethical and clinical principles with the current legal requirements into a 10-step pathway. The pathway emphasises the need for skilful and empathetic communication as central to effective EOL decision-making.
The way forward
Several state health ministries have taken steps to implement the Supreme Court Judgement - Jan 2023. They include Maharashtra, Karnataka, Goa and Haryana. There is a rapidly growing physician and public awareness of the need to promote dignified death. Campaigns to facilitate execution of Living Wills are also underway. What is needed is for physicians to champion the cause of ethical decision-making on the ground in every healthcare environment.
To cite
: Mani R K. End-of-Life Care in India. Indian Transplant Newsletter. 2025 Apr-Jun; 24(2):p4-5.
DOI: 10.64384/ITN.2025.034
Available at:
https://www.itnnews.co.in/indian-transplant-newsletter/issue76/End-of-Life-Care-in-India-1404.htm
Available at:
https://www.itnnews.co.in/indian-transplant-newsletter/issue76/End-of-Life-Care-in-India-1404.htm
- Copyright © 2026. Published by MOHAN Foundation
