Home / Newsletters / ITN 64 / Subscribe
First report of Domino Liver Transplant from India
Avnish Seth, Neha Sharma, Sukhvinder Lal
Indian Transplant Newsletter. 2021 Nov - 2022 Feb; 21(Cumulative issue 64):p7
Print ISSN 0972 - 1568
Online ISSN 3048 - 653X
Download PDF
Dr Avnish Seth, Ms Neha Sharma, Ms Sukhvinder Lal
Domino liver transplant (DLT) is performed by using the explanted liver of a liver transplant recipient as the donor graft in another patient. This is usually feasible when liver transplant is performed in the initial recipient for hereditary metabolic disorders like familial amyloid neuropathy. The explanted liver, which is structurally normal, is then transplanted into another patient, usually with liver malignancy. The first domino liver transplant was done in India recently, but in very different and unusual circumstances.
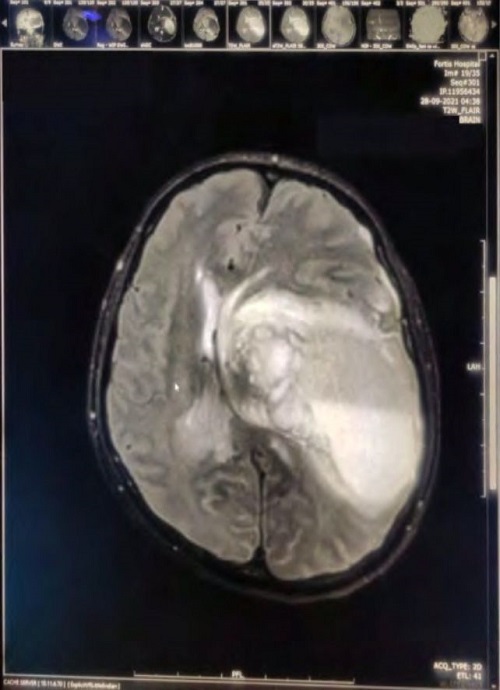
Mr ABC (name changed), 53 years, underwent a deceased donor liver transplantation for decompensated cirrhosis of liver due to auto-immune hepatitis at Fortis Memorial Research Institute, Gurugram, in September 2021. The donor, a 44 years old lady, was declared brain dead in the same hospital following brain hemorrhage due to ruptured aneurysm. Mr ABC was doing well post liver transplant with good graft function. Unfortunately, on Day-6 following liver transplant, while still in ICU, he developed sudden loss of consciousness with generalized seizures. MRI brain revealed massive intra-cranial bleeding (fig). Soon he developed signs of brain stem dysfunction in the form of non-reactive pupils and absent cornea and gag reflexes. The first set of tests for brain death, including the Apnea test, carried out by the brain death committee, were suggestive of irreversible brain stem damage. The family was counseled on the unfortunate turn of events by the liver transplant and ICU teams. Over the following 5 days, the family was repeatedly counseled on the opportunity for organ donation by a team approach. At least three members were always present for the counseling, viz. from medical administration, transplant coordination and one expert by rotation from critical care / neurology / neurosurgery. The family, shocked by the sudden turn of events, took their time to decide on donation. Meanwhile, the critical care team continued the donor maintenance protocol and the second set of tests for confirmation of brain death were done.
On the 5th day of counseling, when the family consented to donation of kidneys and the liver, the donor was not on inotropes, BP 150/90 mm Hg, pulse 80/minute, Hb 7 G/dl, WBC count 25,620 /cmm, X-ray chest was normal, blood culture sterile, creatinine 1.02 mg/dl, sodium 145 meq/L, potassium 3.42 meq/L, bilirubin 1.0 mg/dL, AST 49 U/L, ALT 151 U/L. Retrieval of both kidneys and the transplanted liver were done 7 days, 23 hours and 49 minutes after the diagnosis of brain death.
The liver was allotted by NOTTO to a hospital in the NCR. This was the first time in the country that a previously transplanted liver was up for allotment. Most prospective recipients from liver transplant centers in the NCR, when offered the liver, expressed uncertainty and concern with likely outcome of using such a liver and opted against transplantation. Fortunately, the team at Max Hospital, Delhi, were able to find a suitable recipient who was willing to accept the previously transplanted liver. The surgery was successful and the recipient did well post operatively and continues to do well at 5 months follow-up.
To cite
: Seth A, Sharma M, Lal S. First report of Domino Liver Transplant from India. Indian Transplant Newsletter. 2021 Nov - 2022 Feb; 21(Cumulative issue 64):p7.
Available at:
https://www.itnnews.co.in/indian-transplant-newsletter/issue64/First-report-of-Domino-Liver-Transplant-from-India-1151.htm
Available at:
https://www.itnnews.co.in/indian-transplant-newsletter/issue64/First-report-of-Domino-Liver-Transplant-from-India-1151.htm
- Copyright © 2026. Published by MOHAN Foundation
